CT Coronary Angiogram And Calcium Score
Background
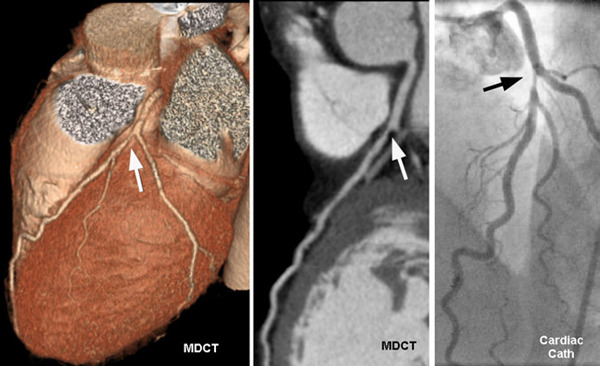
A computerized tomography (CT) coronary angiogram is an imaging test that looks at the arteries that supply blood to your heart. It might be used to diagnose the cause of chest pain or other symptoms.
A CT coronary angiogram relies on a powerful X-ray machine to produce images of your heart and its blood vessels. These tests are noninvasive and don't require recovery time. Coronary CT angiograms are increasingly an option for people with a variety of heart conditions.
Why it is done?
A coronary CT angiogram can check your heart for various conditions, but it's primarily used to check for narrowed or blocked arteries in your heart (coronary artery disease). If your test suggests that you have heart disease, you and your health care provider can discuss treatment options.
Risks
You'll be exposed to some radiation during the test. The amount varies depending on the type of machine used. The risk of developing cancer from a CT angiogram isn't known, but it's small. However, you shouldn't have a CT angiogram if you're pregnant because of possible harm to your unborn child.
It's possible that you could have an allergic reaction to the dye used in the procedure. Talk to your doctor if you're concerned about having an allergic reaction.
Prepration
Your doctor should give you instructions about how to prepare for your CT angiogram. You can drive yourself to the appointment, and you'll be able to drive after your test.
Food and medication
Usually, you'll be asked not to eat anything for about four hours before your test. You can drink water, but avoid caffeinated drinks 12 hours before your test, because they can increase your heart rate, which can make it difficult for your doctor to get clear pictures of your heart. If you're allergic to the dye used in the procedure, your doctor might ask you to take steroid medication 12 hours before the procedure to reduce your risk of a reaction.
Clothing and personal items
You'll need to remove clothing above your waist, as well as jewelry and glasses, and change into a hospital gown.
Before the procedure
Your doctor might give you a medication called a beta blocker to slow your heart rate, enabling the scan to produce a clearer image. Let your health care provider know if you've had side effects from beta blockers in the past.
You might also be given nitroglycerin to widen (dilate) your coronary arteries. If you're allergic to contrast material, you might be given medication to lower your risk of a reaction.
During the procedure
A technician will give you numbing medication before inserting an intravenous (IV) line in your hand or arm to inject the dye that will make your heart's arteries visible on the images. Although the actual scanning portion of the test takes as few as five seconds, it may take up to an hour for the whole process.
The technician will place electrodes on your chest to record your heart rate. You'll lie on a long table that slides through a short, tunnel-like machine. During the scan you'll need to stay still and hold your breath so as not to blur the images. If you're uncomfortable in closed spaces, ask your doctor if you need medication to help you relax.
A technician will operate the machine from a room that's separated from your exam room by a glass window. There will be an intercom system that allows you and the technician to communicate with each other.
After the procedure
After your CT angiogram is completed, you can return to your normal daily activities. You should be able to drive yourself home or to work. Drink plenty of water to help flush the dye from your system.
The images from your CT angiogram should be ready soon after your test. Usually, the health care provider who asked you to have a CT angiogram should discuss the results of the test with you.
Results
Based on the results of your test, your health care provider will discuss with you whether you have a heart condition that needs treatment, whether you're at risk of developing heart disease and steps you can take to keep your heart healthy.
Regardless of the results of your test, it's a good idea to make lifestyle changes to help protect your heart. These include:
•Exercise regularly. Exercise helps you reach and maintain a healthy weight and control diabetes, elevated cholesterol and high blood pressure — all risk factors for heart disease. With your doctor's OK, aim for 30 to 60 minutes of moderate to vigorous physical activity most days of the week. If necessary, break your activity into several 10-minute sessions a day.
•Eat healthy foods. A heart-healthy diet based on fruits, vegetables and whole grains — and low in saturated fat, cholesterol and sodium — can help you control your weight, blood pressure and cholesterol.
•Stop smoking. Smoking is a major risk factor for heart disease, especially atherosclerosis. If you smoke, quitting is the best way to reduce your risk of heart disease and its complications.
•Maintain a healthy weight. Excess weight can contribute to high blood pressure, abnormal cholesterol levels and type 2 diabetes. Losing weight, even a small amount, lessens these risks.
•Manage health conditions. If you have high blood pressure, elevated cholesterol or diabetes, take your medications as directed. Ask your doctor how often you need follow-up visits.
•Manage stress. Stress can cause your blood vessels to constrict, upping the odds of a heart attack. Ask your doctor about stress management programs in your area. Exercise can help reduce stress too.
Cardiovascular disease (CVD) is the leading cause of death in the United States, where up to 60 percent of adults will have a myocardial infarction, stroke or incident of heart failure in their lifetimes. Despite these striking numbers, research data suggest that CVD is largely preventable. Individuals with an optimal risk profile — collectively named "Life's Simple 7" by the American Heart Association — have as much as an 80 percent reduction in risk of CVD.
Cholesterol and CVD risk
Six of Life's Simple 7 (healthy diet, physical activity, no smoking, and well-controlled blood pressure, blood glucose and body weight) can be universally recommended by clinicians. However, the seventh item (cholesterol level) is a challenge because the optimal level is primarily determined by an individual's risk of CVD.
National guidelines recommend the use of population-based risk algorithms, such as the Pooled Cohort Risk Assessment Equations, to determine atherosclerotic cardiovascular risk (ASCVD). "These risk algorithms are remarkably effective in predicting risk in populations, but have limitations in predicting individual risk," says R Todd Hurst, M.D., director of the Heart Health and Performance Program at Mayo Clinic's campus in Phoenix/Scottsdale, Arizona. "The best illustration of these limitations is that the majority of CVD events (up to 75 percent) occur in low- and intermediate-risk populations."
Because more-accurate means of determining individual CVD risk are needed, a search is ongoing for better tools to identify high-risk individuals before clinical events occur. One such tool is imaging for subclinical atherosclerosis, most commonly accomplished by quantifying the amount of calcium in the coronary arteries by computerized tomography.
Subclinical atherosclerosis and CVD risk prediction
The coronary artery calcium score (CACS) is strongly correlated with future risk of myocardial infarction and stroke, making it a potentially attractive tool to further clarify individual risk of CVD. Several large studies with long-term follow-up have shown that CACS adds incremental information in CVD risk identification and provides more-accurate CVD risk prediction compared with traditional risk factors in about 25 percent of individuals.
Despite the potential utility of these data, it is not known if identifying individuals who are at higher risk by CACS — and intensifying the prevention regimen — lowers the risk of CVD events. That question has not been adequately studied.
What patient should not have a CACS?
The appropriate patient for CACS is still debated, and the answer to this question will likely continue to evolve as data accumulate. However, there is more agreement among experts in CVD prevention concerning patients for whom CACS is rarely indicated:
- Patients with clinical CVD or those already taking a statin medication
- Patient scenarios where both the clinician and the patient agree that a statin is indicated
- Patient scenarios where both the clinician and the patient agree that a statin is not indicated
- Patients who have had previous CACS to assess the response to treatment
What patient should have a CACS?
While there is not enough evidence to make a recommendation without reservation to perform CACS in any patient, many clinicians who specialize in CVD prevention (including those at Mayo Clinic) believe that CACS can add valuable clinical information in selected patients.
At Mayo Clinic's campus in Arizona, the most common indication for CACS is lack of a decision by the patient, the clinician or both about whether to start a statin for CVD risk reduction. In such a situation, the imaging study can further clarify the patient's risk and, by extension, whether a statin medication should be considered. There are several common clinical scenarios where the individual's risk of future CVD is uncertain:
Family history of CVD
Family history is often the most difficult CVD risk factor to assess. Although it is clear that family history is an important determinant of risk, the complex interplay between genetic factors, environmental exposure and lifestyle choices often makes confident assessment of an individual's risk impossible. In this situation, CACS may help determine if the patient has a genetic disposition to atherosclerosis.
Striking risk factor in a young patient
Because age is the most heavily weighted factor in population-based risk algorithms, younger patients (younger than 60 years) are less likely to be high risk, even if they have significant risk factors. The guidelines recommend considering a lifetime risk score in such patients. However, many clinicians use CACS to guide prevention recommendations.
'Gray zone' (5 to 7.5 percent) ASCVD 10-year risk score
An imaging study may place the patient in either a lower or a higher risk category that would then impact clinical recommendations.
What Is A High-Risk Imaging Result?
CT of patient with CACS of 4,410 Agatston units
The generally accepted definition of high risk with CACS is a reading higher than 300 Agatston units or a CACS at or above the 75th percentile when adjusted for age, sex and race.
Too much or too little?
The answer to the question "Are we doing too many CACS studies or too few?" is primarily dependent on the clinical judgment of each clinician. "It is clear that there is great need to more accurately identify individuals who are at high risk of CVD prior to clinical events, yet the role of CACS in CVD risk prediction, if any, is not clearly defined from the current data," says Dr. Hurst.
Until more-definitive data become available, most experts in prevention of CVD favor a strategy that limits use of CACS to those patients for whom the result would have the most impact on treatment recommendations.
CT Coronary Angiogram & Calcium Score
What is a CT coronary angiogram?
- CT stands for computed tomography, a type of imaging test that provides 3-D images of your organs, blood vessels and other tissues.
- A CT coronary angiogram uses CT technology to look inside the arteries that supply blood to your heart.
- Unlike traditional angiograms that use a catheter inserted into your arteries, a CT scan is completely noninvasive, which means the doctor can see inside your arteries without any incisions.
What happens during a CT coronary angiogram?
- CT scans use a powerful x-ray machine to produce images of the inside of your body.
- During a CT coronary angiogram, you'll lie on a special platform that will move you through the CT scanner.
- As you move, the x-ray device will rotate rapidly around you, creating a series of 3-D images that provide the doctor with an in-depth, detailed look at your coronary arteries.
- During portions of the scan, you may be asked to hold your breath so the scanner can gain more detailed images. Most scans take about 10 minutes to complete.
What is calcium scoring?
Calcium scoring is a recently developed technique for identifying calcified plaque in the coronary arteries. Plaque buildup is the primary cause of arterial blockage that slows the flow of blood to your heart. It's also a primary cause of chest pain, or angina, and heart attack. In calcium scoring, a CT angiogram is performed to evaluate the presence and location of plaque in your coronary arteries. Those findings are interpreted as a calcium “score” that can determine the presence of coronary artery disease (CAD) as well as your risk of heart attack or other complications. Scores range from 0 (no evidence of CAD) to 400 (extensive evidence of CAD). Calcium scores can also be helpful to determine if a specific treatment is working as it should.
The first Rumberger guideline based on Agatston score using Electron Beam Computed Tomography (EBCT)
Calcium Score |
Presence of plaque |
|---|---|
0: |
No plaque is present. You have less than a 5% chance of having heart disease. Your risk of a heart attack is very low. |
1 – 10: |
A small amount of plaque is present. You have less than a 10% chance of having heart disease. Your risk of a heart attack is low. However, you may want to quit smoking, eat better, and exercise more. |
11 -100: |
Plaque is present. You have mild heart disease. Your chance of having a heart attack is moderate. Talk with your doctor about quitting smoking, eating better, beginning an exercise program, and any other treatment you may need. |
101-400: |
A moderate amount of plaque is present. You have heart disease, and plaque may be blocking an artery. Your chance of having a heart attack is moderate to high. Your health professional may want more tests and may start treatment. |
> 400: |
(extensive evidence of CAD). May require invasive coronary angiography |
Summery of CT calcium score
0 none
1–99 mild
100–400 moderate
>400 severe
*Calcium score correlates directly with risk of events and likelihood of obstructive CAD*